HOME > Research Summaries > Analysis of Composition and Mechanical Stress of Vessels from 4D-data by dual MDCT: Radiological anatomy of the right adrenal vein
Research Summaries

Analysis of Composition and Mechanical Stress of Vessels from 4D-data by dual MDCT: Radiological anatomy of the right adrenal vein
Shoki Takahashi*, Kei Takase, and Tomonori Matsuura
Professor
Department of Diagnostic Radiology, Graduate School of Medicine
E-mail:![]()
Abstract
As an example to study minute vessels with multi-detector row computed tomography (MDCT), we determined how frequently the right adrenal vein (RAV) could be identified on MDCT and what spectrum of anatomic variations was seen among the RAVs visualized.
Post-contrast MDCT obtained in 104 patients were reviewed. Regarding the RAV, we evaluated the degree of visualization; the relationship to other veins; the anatomy in relation to the surrounding structures, direction, length and diameter. The RAV was detected in 76% of the patients. The orifice was craniocaudally located between the level of vertebrae T11 and L1. Among the 73 patients, the RAV joined the inferior vena cava (IVC) in the right posterior quadrant in 71 and in the left posterior quadrant in 2 patients. The vertical direction from the IVC was caudal in 65 and cranial in 8 patients.
MDCT enabled the identification of the RAV and delineation of its anatomy, including the position and relationship to surrounding structures.
1. Introduction
We have analysed high resolution images of various vessels by using a multi-detector CT (MDCT, single X-ray tube). As one of such examples, we present here a study on radiological anatomy of the right adrenal vein.
Primary aldosteronism is the most common form of secondary hypertension, and its prevalence in hypertensive populations is estimated at approximately 10% [1]. Unilateral aldosterone-producing adenoma and bilateral idiopathic hyperaldosteronism are the two most common subtypes of primary aldosteronism, and distinguishing between them is critical for treatment planning, because the former is treated with adrenalectomy while the latter is treated medically. CT and MRI are both still unreliable methods for distinguishing the subtypes of primary aldosteronism, for which adrenal venous sampling is often undertaken [2].
Selective adrenal venous sampling can be difficult to perform because catheterization of the right adrenal vein (RAV) generally remains difficult [3], whereas catheterization of the left adrenal vein is a simple procedure.
MDCT could possibly guide adrenal venous sampling if it were capable of delineating the anatomy of the RAV. Although Daunt referred to the feasibility of identifying the RAV with MDCT [12], to our knowledge, a detailed analysis regarding visualizing the anatomy of the RAV with MDCT has never been made. We undertook this study to determine how frequently the RAV could be identified on MDCT and what spectrum of anatomic variations was seen among the RAVs.
2. Materials and Methods
2. 1. Acquisition of CT images
We performed a retrospective analysis of CT images from 104 consecutive patients. The CT scanner was an Aquilion 8-detector row helical CT scanner (Toshiba, Tokyo, Japan).
2.2. Points of evaluation
The rate of visualization and number of the RAV were checked. The craniocaudal level of the RAV orifice was specified relative to vertebral bodies and discs. The position of the orifice was also evaluated along the circumference of the IVC as an angle Q in the x-y plane. To evaluate the direction of the RAV at the branching portion from the IVC, the angle between the RAV and x-axis (angle 1) and the craniocaudal angle between the RAV and z-axis (angle 2) were measured. We measured the length of the RAV between the exit from the right adrenal gland and entry to the IVC, and the diameter of the RAV at the junction with the IVC.
3. Results
The RAV was detected in 79 (76%) of 104 patients, in which the following anatomical analyses were made (Fig. 1). Among the 79 patients with an identifiable RAV, the RAV and accessory hepatic vein formed a common trunk before entering the IVC in 6 (8%), the RAV entered the IVC directly but almost shared a common orifice with an accessory hepatic vein in 7 (9%), and the RAV entered the IVC independently of other vein in the remaining 66 (84%) patients. In 50 (69%) of the 73 patients, the RAV joined the IVC at the level ranging from the middle third of T12 to the superior third of L1 (Fig. 2). Angle Q ranged from -7 degree to 71 degree (mean, 39 degree; SD, 16 degree). The angle 1 ranged from -36 degree to 47 degree (mean, 8 degree; SD, 18 degree). The angle 2 ranged from 30 degree to 136 degree (mean, 73 degree; SD, 23 degree) (Fig. 3). The mean length was 3.8 ± 1.7 (SD) mm, and the mean diameter at the junction with the IVC was 1.7 ± 0.6 (SD) mm.
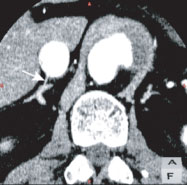
Fig. 1. A 56-year-old man with an aortic dissection. A para-axial multiplanar reconstruction (MPR) image shows excellent visualization of the right adrenal vein (RAV, arrow) running through the intervening adipose tissue to join the right posterior quadrant of the inferior vena cava. The length of the RAV was 8 mm.
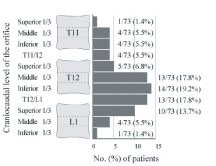
Fig. 2. The craniocaudal level of the right adrenal vein (RAV) orifice in relation to the vertebrae.
4. Conclusion
MDCT enabled the identification of the RAV and delineation of its anatomy, including the position and relationship to the surrounding structures such as the IVC in a high percentage of patients and this preoperative information, when obtained, would help perform the catheterization of the RAV for adrenal venous sampling.
5. Perspective
Recently-developed MDCT having two X-ray tubes with different KVp may provide us a unique way of analysis of vessel wall. Analysis of the composition and mechanical stress of diseased vessels from 4D-data obtained by dual MDCT would provide insights to the mechanism of disease processes and posttherapeutic recurrence, which would in turn enable us to non-invasively diagnose and treat vascular diseases.
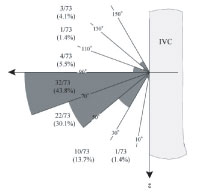
Fig. 3. The craniocaudal angle of the right adrenal vein with z-axis in the vertical plane.
IVC = inferior nena cava.
Acknowledgements
We acknowledge the support of Tohoku University Global COE Programme "Global Nano-Biomedical Engineering Education and Research Network Centre".
References
[1] Gordon RD, Stowasser M, Tunny TJ, Klemm SA, and Rutherford JC. High incidence of primary aldosteronism in 199 patients referred with hypertension. Clin Exp Pharmacol Physiol 21(4), 315-318, 1994.
[2] Young WF, Stanson AW, Thompson GB, Grant CS, Farley DR, and van Heerden JA. Role for adrenal venous sampling in primary aldosteronism. Surgery 136(6), 1227-1235, 2004.
[3] Espiner EA, Ross DG, Yandle TG, Richards AM, and Hunt PJ. Predicting surgically remedial primary aldosteronism: role of adrenal scanning, posture testing, and adrenal vein sampling. J Clin Endocrinol Metab 88(8), 3637-3644, 2003.